
This is the first of a series of posts analyzing payer-published provider directory data sets mandated by the CMS Final Rule. Defacto Health is accumulating data from payers’ provider directory APIs to assist in in-network provider search and related use cases. The first question we are posing is “how prevalent are centralized appointment phone numbers?” As an increasing number of practitioners work for health systems, many provider data professionals have observed that system-wide appointment scheduling phone numbers are being listed across many locations and practitioners in payer directories.
Benefits of Centralized Appointment Scheduling
Centralized appointment call center can more scalably handle inbound scheduling requests from patients and can allow those closer to the practice to focus more on patient care. These call agents theoretically have access to the schedules and physical locations of every practitioner in the health system and can help navigate the patient to the right in-network practitioner at the right location in a timely fashion.
Risks in Centralized Appointment Scheduling
Depending on the health system, its “source of truth” for schedule and location data may be more or less accurate. Sometimes practices that have been recently acquired by a health system are still functioning within a silo separate from the rest of the system. For example, my family practice in Northern Virginia was acquired by a large health system. I used the health system’s appointment scheduling feature to book an appointment and even received a confirmation e-mail. I called into the practice itself about a week out to confirm my appointment, and the agent said “oh, we’re not plugged into their system yet. your appointment wasn’t booked.” If an integrated source of truth hasn’t been established, then a centralized function might provide less-than-accurate information, because the agent is physically removed from the practice. On the other hand, if investments have been made, centralized appointment systems could be a valuable resource for payers, if they are able to collaborate with the health system to gain access to the supporting data repositories.
The Implications of Centralized Appointment Phone Numbers
The prevalence of centralized phone numbers could have an impact on payer directories, and could inform the style of interventions employed to solve for quality issues. If these phone numbers represent a large percentage of overall records within a health plan’s directories, then it may be worthwhile to take a system-by-system approach to assess provider directory data quality and collaborate with the health system on interventions. It also reveals the limitations for telephonic audits on those health systems, as centralized call centers can build rapid defenses against regulatory and payer-driven data quality telephone calls (e.g., blackhole voicemail boxes for inbound audit calls). Finally, to the extent those health systems have centralized appointment functions with accurate information, these present opportunities for collaboration to source high quality directory data.
Methodology for Assessing the Prevalence of Centralized Appointment Phone Numbers
Defacto Health analyzed data aggregated from 10 health plans: 6 nationals and 4 state blues. We normalized and matched phone numbers and addresses that are published in directories for all of those health plans. On this normalized data set, we queried on a random sample of unique phone numbers across all directories, and determined how many addresses and practitioners are associated with those unique phone numbers.
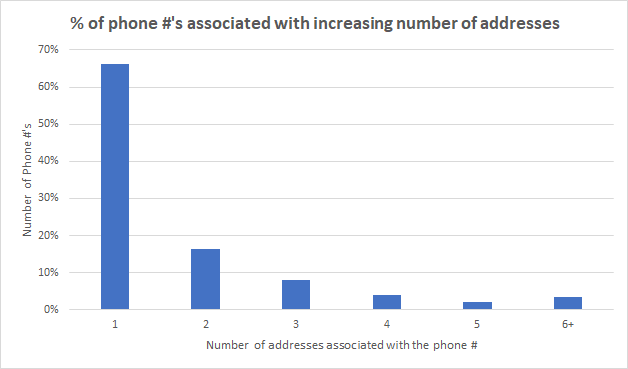
Number of addresses associated with unique phone numbers
The graph below shows the prevalence of phone numbers with a increasing number of addresses associated with them. For our purposes, we can consider those phone numbers with more than three addresses as ‘centralized’ (i.e., agents may be present at one location, but would be physically separated from others). A majority (66%) of phone numbers are associated with just one address, so it is likely that the phone is “local” (however, it could be a larger campus with many departments and practitioners at a single address). 18% of phone number are associated with 3 or more physical addresses.
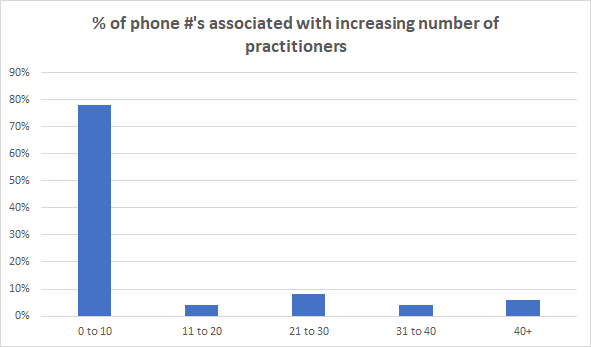
Number of practitioners associated with unique phone numbers
The analysis on practitioners associated with phone numbers shows a similar distribution. The majority of phone numbers are associated with up to 10 practitioners (i.e., an agent could keep on top of the locations of 10 practitioners at a single practice), however 22% of phone numbers are associated with more than 10 practitioners in a payer’s directory. Given that greater than 70% of physicians now work for hospitals, one could anticipate a future trend towards greater centralization, even for those practices currently publishing their own phone numbers and scheduling their own appointments.
Takeaways
There is a significant percentage (between 18% and 22%) of ‘centralized’ phone numbers published within health plan provider directories. The clusters of these directory records represent an opportunity to assess directory data quality on a health system-wide basis. When the data is accurate via these appointment functions, then there is an opportunity for payers to work with those health systems to source this accurate data. When the data is less accurate, then this represents an opportunity to collaborate in a scalable way with health systems as they establish their patient access ‘source of truth’ (working on their own provider search and appointment functions). Regulators should be careful as they audit information telephonically via centralized appointment phone numbers, as the accuracy of the information provided can vary.